Patients with rheumatic disease who are immunosuppressed or have significant comorbidities are at increased risk for serious infection. The COVID-19 pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, is of particular concern for these patients. Rheumatic disease and/or an immunocompromised status may place patients at higher risk for a more severe course of COVID-19, including complications, hospitalization, and death.1
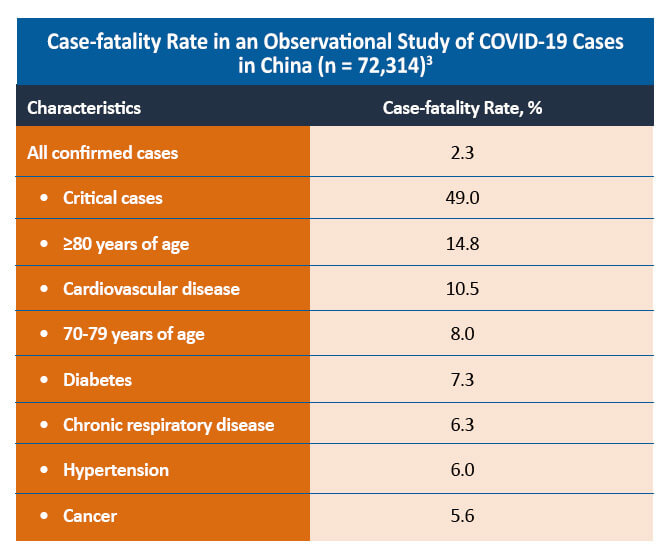
Epidemiologic studies have found that patients with significant comorbidities, including cardiovascular disease, hypertension, and diabetes, are at increased risk for developing severe complications with COVID-19 infection. Current research is investigating the risk of severe COVID-19 in patients with PsA as the disease is associated with a higher incidence of comorbid cardiovascular disease, metabolic syndrome, obesity, diabetes mellitus, dyslipidemia, and inflammatory bowel disease.2
A comparative cohort study of patients with and without rheumatic disease found that both groups of patients had similar symptoms and laboratory findings. Although a similar proportion of patients with and without rheumatic disease was hospitalized in the study (44% vs 40%; P=0.50), patients with rheumatic disease were more likely to require intensive care admission and mechanical ventilation (48% vs 18%). The mortality rate was similar between the two groups (6% vs 4%; P=0.69).4
However, a small cohort study in Italy found that the presence of rheumatic disease or the degree of pharmacologic immunosuppression did not differ between patients with confirmed or suspected COVID-19 and those without. In this study, poor outcome was associated with older age and the presence of arterial hypertension and obesity.5 A large cohort study of 456 rheumatic and non-rheumatic patients found that chronic inflammatory arthritis or previous immunosuppressive therapies did not increase the risk of death, invasive ventilation, intensive care unit admission, or serious complications from COVID-19. However, older age, male sex, and previous comorbidity (obesity, diabetes, hypertension, cardiovascular or lung disease) were associated with increased risk in the rheumatic cohort.6
Treating PsA During the COVID-19 Pandemic
An additional concern for rheumatologists is the impact of PsA therapy on the risk of SARS-CoV-2 infection or the development of severe COVID-19. A case series of individuals with rheumatic disease and COVID-19 from the COVID-19 Global Rheumatology Alliance registry investigated the rate of hospitalization for COVID-19 in patients with rheumatic disease. The study found that a prednisone dose >10 mg/day was associated with a higher risk of hospitalization (OR, 2.05). However, use of conventional disease-modifying antirheumatic drugs (DMARDs) alone or in combination with biologics or Janus kinase inhibitors was not associated with an increased risk of hospitalization. No association between hospitalization and non-steroidal anti-inflammatory drugs (NSAIDs) or antimalarial use was observed. Tumor necrosis factor inhibitor (anti-TNF) use was found to significantly reduce the risk of COVID-19 hospitalization in this study (OR, 0.40).1 Another study in patients with inflammatory bowel disease and COVID-19 found that systemic corticosteroids increase the risk of severe COVID-19 (aOR, 6.9). Anti-TNF therapy was not associated with severe COVID-19 in this study (aOR, 0.9).7
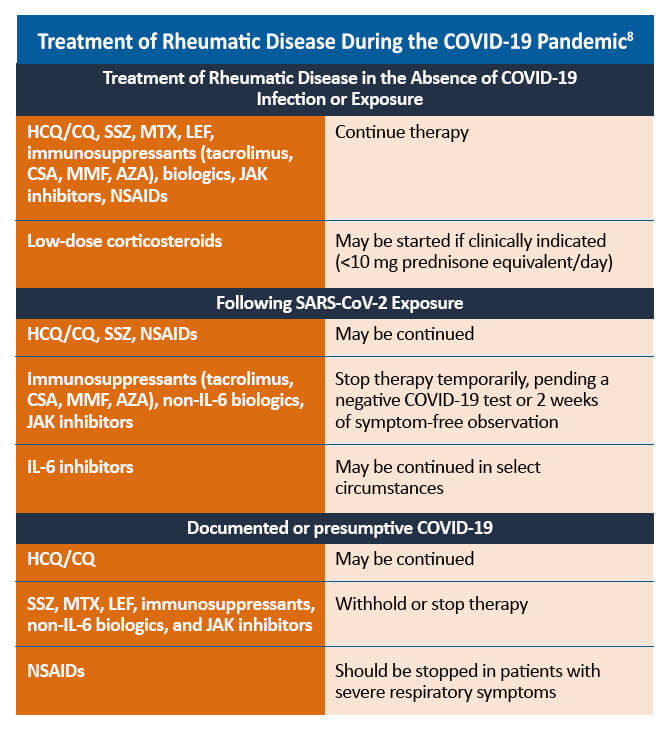
Some therapies for the management of PsA may need to be withheld in patients with confirmed or suspected COVID-19. For patients with uncomplicated COVID-19 infections, such as those who experienced mild or no pneumonia treated in the ambulatory setting or by self-quarantine, therapies to manage rheumatic disease may be reinitiated within 7-14 days of symptom resolution. For patients who are asymptomatic despite a positive PCR (polymerase chain reaction) test for SARS-CoV-2, PsA therapies may be restarted 10-17 days after the positive PCR result. Decisions regarding the timing of reinitiating PsA therapies in patients who recover from more severe COVID-19-related illness should be made on a case-by-case basis.8
References
Gianfrancesco M, Hyrich KL, Al-Adely S, et al. Characteristics associated with hospitalization for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis. 2020;79:859-866.
Wollina U, Fioranelli M, Goldust M, et al. Psoriatic arthritis and COVID-19 pandemic: Consequences in medical treatment? Dermatol Ther. 2020;33:e13743.
Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239-1242.
D’Silva KM, Serling-Boyd N, Wallwork R, et al. Clinical characteristics and outcomes of patients with coronavirus disease 2019 (COVID-19) and rheumatic disease: A comparative cohort study from a US ‘hot spot’. Ann Rheum Dis. 2020;79:1156-1162.
Fredi M, Cavazzana I, Moschetti L, et al. COVID-19 in patients with rheumatic disease in northern Italy: A single-centre observational and case-control study. Lancet Rheumatol. 2020;2:e549-e556.
Pablos JL, Galindo M, Carmona L, et al. Clinical outcomes of hospitalized patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: A multicentric matched cohort study [published online ahead of print, 2020 Aug 12]. Ann Rheum Dis. 2020;218296.
Brenner EJ, Ungaro RC, Gearry RB, et al. Corticosteroids, but not TNF antagonists, are associated with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: Results from an international registry. Gastroenterol. 2020;159:481-491.e3.
Mikuls TR, Johnson SR, Fraenkel L, et al. American College of Rheumatology Guidance for the Management of Rheumatic Disease in Adult Patients During the COVID-19 Pandemic: Version 2. Arthritis Rheumatol. 2020;72:e1-e12.
Updates in the Treatment and Prevention of COVID-19
EUA of Bamlanivimab Plus Etesevimab Expanded to Include Younger Pediatric Patients
The emergency use authorization (EUA) for bamlanivimab plus etesevimab now includes an indication for treatment and post-exposure prophylaxis for children and newborn babies who are at high risk for severe disease. The expansion of the EUA is supported by a trial of 125 pediatric patients with at least one risk factor for severe illness; the study had safety and efficacy data similar to findings for adolescents and adults.
Oral Antiviral Therapies With Emergency Use Authorization (EUA) for COVID-19
Two new oral antiviral therapies received emergency use authorization (EUA) for COVID-19: Paxlovid™ (nirmatrelvir tablets and ritonavir tablets, co-packaged) and molnupiravir. Both therapies are authorized for the treatment of mild-to-moderate COVID-19 in certain people who are at high risk of progressing to severe illness.
In the EPIC-HR clinical trial, nirmatrelvir/ritonavir significantly reduced the risk of hospitalization or death from any cause by 88% compared with placebo. This treatment is indicated for adults and pediatric patients, 12 years of age and older who weigh at least 40 kilograms. Side effects include an impaired sense of taste, diarrhea, high blood pressure, and muscle aches. The safety and effectiveness of this combination therapy continue to be evaluated.
The main outcome measure of the MOVe-OUT trial of molnupiravir was the percentage of people who were hospitalized or died due to any cause during 29 days of follow-up. Compared with 9.7% of people who received placebo, 6.8% of those in the molnupiravir group were hospitalized or died. One person who received molnupiravir died versus nine people in the placebo group. Molnupiravir is not recommended for pregnant women or for those people younger than 18 years of age because of its effect on bone and cartilage growth.
For more information regarding the EUA for these oral antivirals, visit the following FDA URLs:
FDA Authorized Emergency Use Authorization (EUA) for Long-Acting Monoclonal Antibodies as Pre-Exposure Prophylaxis of COVID-19
Evusheld™ (tixagevimab co-packaged with cilgavimab and administered together) has been granted EUA for the prevention of COVID-19 in certain people with compromised immune systems or with a history of severe adverse reactions to a COVID-19 vaccine or any of its components. This combination is not meant to be a substitute for vaccination for those who have no contraindications to a COVID-19 vaccine.
The PROVENT clinical trial demonstrated a 77% reduction in the risk of developing COVID-19 compared with placebo, and protection appears to have been maintained through six months. Safety and efficacy of the tixagevimab/cilgavimab combination continues to be investigated.